
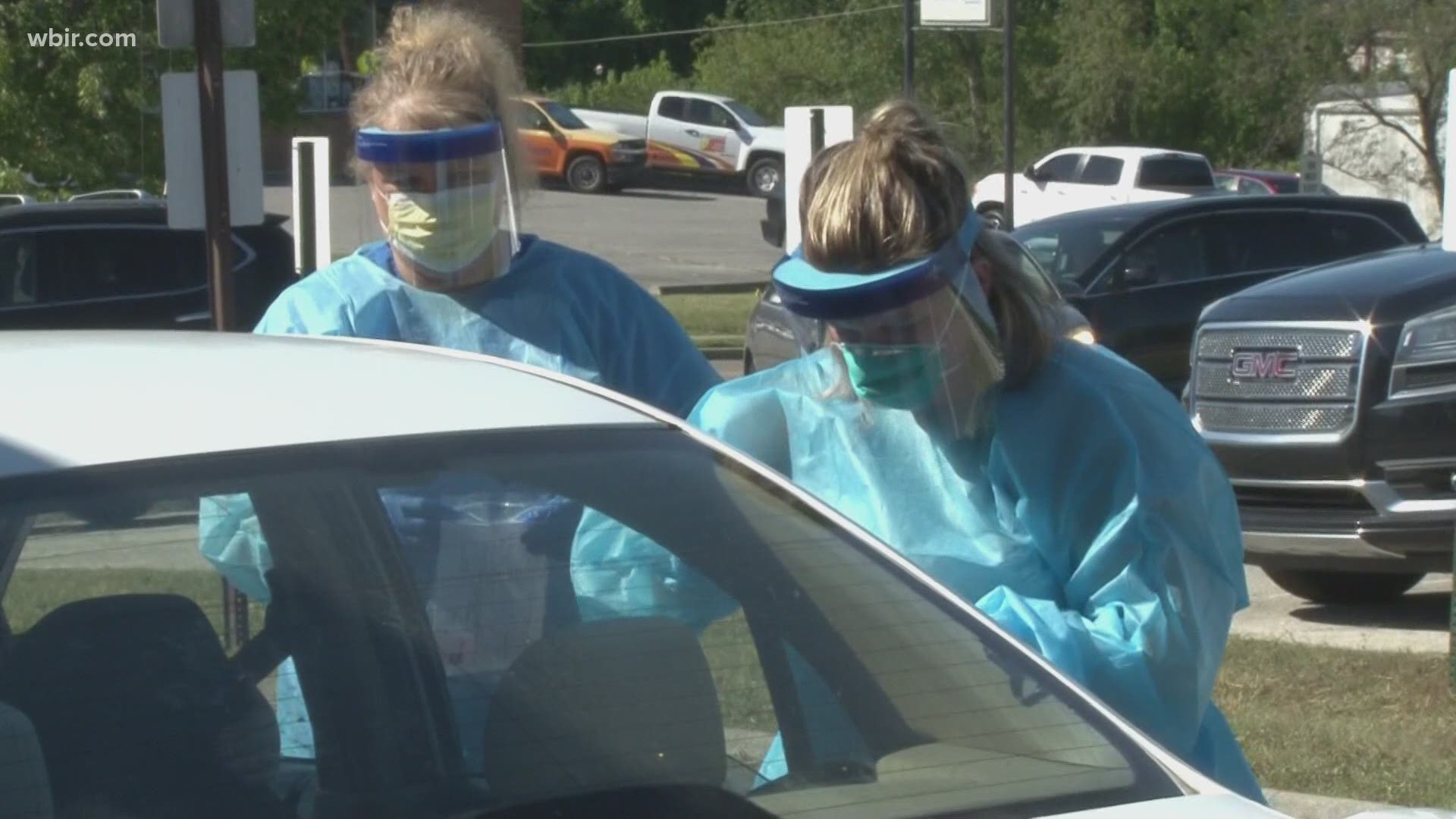
KNOX COUNTY, Tenn. — The fatigue caused by more than half a year of dealing with the daily realities of COVID-19's continued spread has settled in deep for many.
Even though murmurs are growing louder that a novel coronavirus vaccine could be in hand before the end of 2020 – the Knox County Health Department continues to say this is not the time (nor is it ever the time) for people to be careless or flippant about a virus that has so far killed close to 200,000 people in the U.S. and infected millions.
COVID-19 is now spreading in Knox County at record-high numbers a few weeks after the University of Tennessee and K-12 schools resumed in-person classes. In the past week, more than half of the new cases in Knox County are in the 11-20 year-old age group, according to state data. UTK has reported 600 cases since August 19, with all but 8 of them among students.
Public health officials said long before school returned to session that a spike in cases was to be expected, but the high spread among teens and college-age adults recently has led to some downplaying the seriousness of COVID-19, even as public health – particularly those most vulnerable to this virus – remains just as much at risk.
"COVID-19 is all over Knox County, it's not just on campus," Dr. Martha Buchanan, director of the Knox County Health Department, said Tuesday. "It's really important for people to understand and continue to follow those five core actions inside and out."
Most should know the "five core actions" by heart at this point: Wash your hands often, wear a face mask while near others out in public, keep 6 feet of distance from others, sanitize surfaces, and stay at home as much as possible.
The Young Are Strong, Not Invincible
One of the most common misconceptions being spread currently claims in various ways the virus isn't serious or as serious because it's being passed largely among young people right now.
It's very true young people have made up the large majority of cases recently. It's also true healthy young adults and children are statistically at much lower risk of developing any serious complications or symptoms from COVID-19 than the older 'at risk' groups. However, they are not immune to it and remain just as likely to catch it as anyone else.
"Just because you are young and healthy doesn't mean you can't have some complications secondary to COVID-19, and even some long-term effects from that," Buchanan said.
The larger problem with the misconception is that it ignores common factors that significantly raise the risk for severe COVID infections that also exist among many young adults and teens, such as smoking and obesity.
It also ignores the impact unchecked spread would have on community and familial spread. With rising infection rates, younger people now run a greater risk of unknowingly spreading the virus elsewhere in the community if they are careless, as much as they typically would with the seasonal flu or common colds that begin to spread more rapidly after school returns.
"Maybe you're young and healthy and won't have a very bad case, but you'll visit home and visit mom and dad, who may have some chronic medical condition. Or you may visit your grandmother who has some chronic conditions," Buchanan said. "You don't want to put those folks at risk, either."
College students don't live in a campus bubble away from everyone else. They live, commute, shop and work around East Tennessee like everyone else. Outbreaks involving UTK students are not isolated to campus, so a growing number of cases involving students is just as much a cause for concern for the rest of the community.
Herd Immunity
Some people online are also quick to claim the growing number of COVID-19 infections in younger people is "a good thing" because they believe it will speed up herd immunity with little risk to public health. Some also believe "high case counts don't matter" in light of this.
These claims is untrue in the case of COVID-19 based on what is known currently.
Herd immunity is meant to prevent a virus from spreading widely across a community unchecked and protecting most people from developing serious life-threatening symptoms. Health experts continue to say willingly exposing anyone to a virus they lack natural immunity to is a dangerous gamble, and it's a pointless gamble if immune response post-infection does not occur or stay around long enough to ward off reinfections.
The case for "natural immunity," which is immune protections after contracting COVID-19, is a mixed bag currently. However, studies into people's natural immunity to COVID-19 are bearing fruit to help develop an effective vaccine.
One recent study showed the COVID-19 antibodies that provide immune protections can decay quickly after people recover from mild infections, which would suggest strategies of obtaining natural herd immunity through infection would be fruitless. However, all studies are incredibly limited on the length of time they can observe people given the virus has been around for less than a year.
Another study out of Iceland this month provides some hope people's COVID-19 immune response could last at least few months after infection, but ultimately highlights the problem that the more serious infections have been a primary trigger for seeing better immune responses in people who recover.
Studies on T cell response to COVID-19 are making the most promising case that natural immunity is possible in the long-term, even for people who only had mild infections. One study was limited by only having a small group of infected people to work with, but found T cells responded in a robust way in many cases to ward off COVID-19 -- even when B cell antibodies were not detected in people who had asymptomatic or mild cases. This suggests the T cell response to COVID-19 could provide a level of immunity to fight off recurrent infections even if antibodies aren't present to neutralize it.
However, Dr. Buchanan said people need to remember there is still a critical lack of long-term observation and data on post-infection "natural" immunity to COVID-19 or its ability to reinfect people, saying current evidence is still pointing more toward short-term immune responses in most people.
"We think it’s pretty short lived, maybe 3 months – maybe a little more, so that is not going to protect us very long," she said.
She believes herd immunity will only be possible through vaccines, and those vaccines are being designed with the goal of triggering both prolonged antibody and T cell immune responses to the virus without the risks that come with being infected.
Multiple vaccine trials are moving through the pipeline, and Governor Bill Lee said he believes the first round of vaccines in Tennessee could be available to the public as early as November. He said he was "encouraged" after federal officials told state leaders to prepare a plan to distribute vaccines by November or December.
What that vaccine will look like and what its capability to immunize against COVID-19 will be remain unknown until at least one finishes its final round of tests and is approved, but Buchanan said she believes KCHD is well-prepared to handle rapid demand for vaccinations once they have them in hand. KCHD said it intends to work with local providers to help increase the availability of vaccines to people once they are available.
It's Not "Just Another Cold"
An oft-repeated lie or misconception spread during the early weeks of the COVID-19 pandemic that downplayed its seriousness was that it was "just the flu." Six months later, COVID-19 is already positioned to be one of the top leading causes of death in the U.S. in 2020, claiming many times more lives in the span of just half a year than multiple strains of the flu typically claim in a full year.
A similar misconception has people claiming recent infections in schools are "just another cold," or "only as bad as the cold." Some go as far as to incorrectly say the current confirmed COVID-19 cases at schools and college campuses are actually common cold strains of the coronavirus instead of COVID-19.
While common cold coronaviruses and COVID-19 have similar mild symptoms and patterns of spreading, the tests used to detect and confirm active positive cases of COVID-19 are only testing for that particular strain of coronavirus.
The Centers for Disease Control said PCR testing, which is the nasal swab test that's been used most commonly, only tests for COVID-19. The PCR test itself looks for specific segments of DNA unique to COVID-19 to obtain the sample's "DNA fingerprint." If it tested a strain of the "common cold" coronaviruses, the DNA fingerprint would not match and the test would come back negative.
Of course, these tests do not come with a 100% certainty of accuracy. No test does no matter how accurate it is because there are multiple chances for errors to happen along the way, such as cross-contamination or having a poor swab sample. This can and will lead to chances for both false positives and false negatives, however the chances of either happening are low.

It's Not Just "6%"
Last month, some people online took a weekly data report from the CDC out of context and conflated data on comorbidities to incorrectly report "94% of people who died from COVID-19 had underlying conditions." That led many others to wrongly believe or claim only 6% of reported deaths were due to COVID-19.
Neither claim is true. For 100% of the now 169,000 people now listed in the CDC report who died, COVID-19 itself was the condition that inevitably led to their death or contributed to their death. For most, it was the main underlying condition.
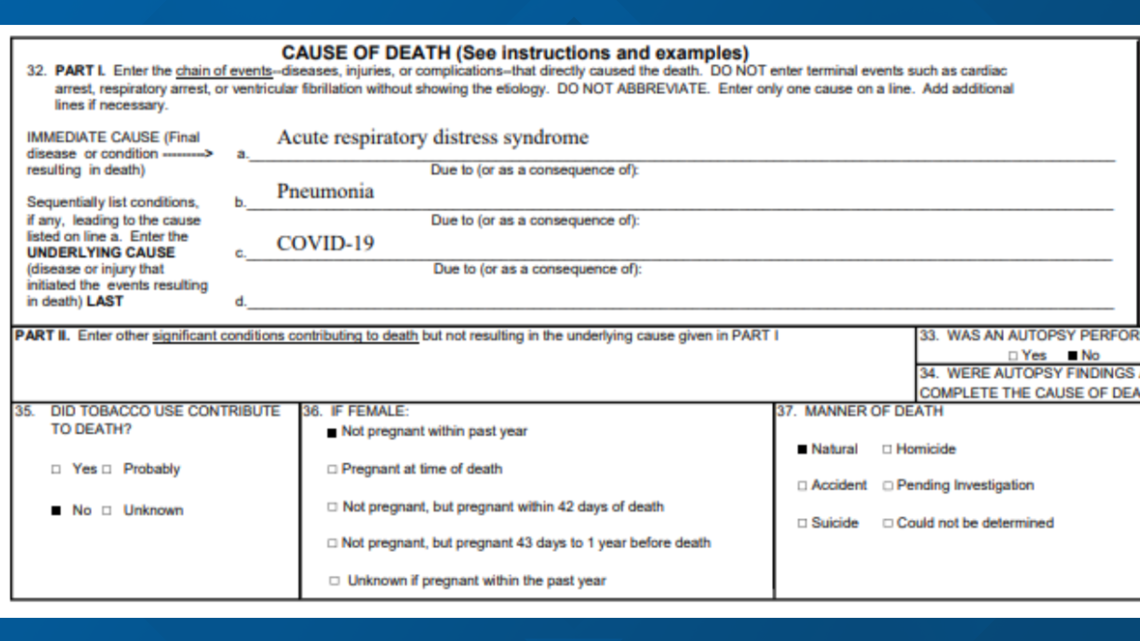
The "94%" figure pulled from the CDC weekly report does not refer solely to "underlying conditions." It's the percentage of people with at least one comorbidity -- something very different. The CDC data includes all conditions contributing to the person's death, including immediate factors such as acute respiratory distress, respiratory failure, and cases of heart failure caused by COVID-19.
So, not all of the 94% had "underlying conditions." COVID-19 itself was the "underlying condition" in many cases, causing the chain of other serious conditions before their death.
It's important to understand how COVID-19 and other conditions are reported in death certificates. The CDC's data is primarily pulled from a person's death certificate, which are filled out by the physician or medical examiner.

The CDC data only includes cases where COVID-19 itself caused or contributed to the person's death. COVID-19 is not supposed to be listed on certificates if a person tested positive but died for completely unrelated reasons, such as a vehicle crash (though this has happened more than once due to human error).
The "6%" number refers specifically to people who died where COVID-19 was the only cause of death mentioned on their death certificates. Those in the "6%" are somewhat outliers when it comes to the virus, as it is well documented COVID-19 frequently causes multiple comorbid conditions in serious cases that can lead to death, particularly respiratory conditions such as pneumonia, acute respiratory distress, and respiratory failure, according to the CDC:
"Inpatient management revolves around the supportive management of the most common complications of severe COVID-19: pneumonia, hypoxemic respiratory failure/ARDS, sepsis and septic shock, cardiomyopathy and arrhythmia, acute kidney injury, and complications from prolonged hospitalization, including secondary bacterial infections, thromboembolism, gastrointestinal bleeding, and critical illness polyneuropathy/myopathy."
In the CDC's most recent weekly data as of September 8 -- of the "94%" with comorbidities, 34% of all COVID-19 deaths involved "respiratory failure," and 42% listed as "pneumonia or influenza."
Conditions such as hypertension and diabetes that are widely noted to be contributing factors to COVID-19 deaths were also noted, but not close to the "94%" many suggest when wrongly assuming all comorbidities were "underlying conditions." As another example, roughly 22% of death certificates included hypertension, and 16% included diabetes.
You might ask, "What was the flu doing there?" This is largely representative of pneumonia alone in the case of COVID-19 comorbidities. The CDC and many other health agencies have grouped the flu together with pneumonia in their reporting for many years, even in cases where pneumonia was caused by something other than the flu. This is because, much like COVID-19 right now, many deaths during flu season aren't from influenza alone, but from influenza-caused pneumonia. The two are combined in reporting to give the CDC and other health experts a more accurate estimate of the flu's true disease burden because the flu has long been underreported on death certificates.